



Yes, your baby needs a Vitamin K shot.
Unless you like head bleeds! This evidence-based injection has saved thousands of lives since 1961. No, the oral version won't work as well.

What if you could ensure your baby did not have a life threatening brain bleed, for several months? What if all it took was one quick, relatively painless injection?
That magical injection exists: the vitamin K shot, which since 1961, has been recommended for all newborns, given as a single intramuscular dose within 6 hours after birth.
This preventive measure has been so successful that Vitamin-K Deficiency Bleeding (VKDB), formerly known as Hemorrhagic Disease of the Newborn, has become incredibly rare - it mostly occurs in those whose parents refuse the shot. But as with the measles vaccine, safety bred skepticism: now the anti-vaxxers and appeal-to-nature influencers encourage parents to forego the vitamin K shot, and in doing so, put their babies in danger of catastrophic, sometimes fatal bleeds.
K is for Koagulation
No, really.
The coagulation cascade is unavoidable on every major medical exam, probably because it is composed of so many annoying names and pathways. Look how annoying:

Luckily for you, you don’t need to encounter it on an 8 hour testing extravaganza. What you need to know is this:
In our bodies, the balance between bleeding and clotting is finely controlled via both pro-bleeding (aka anti-coagulant) and pro-clotting (prothrombotic or procoagulant) factors.
In the course of normal life, our blood vessels experience damage all the time, and we want the body to be able to stop smaller bleeds from becoming bigger ones by making little thrombi (plugs) to repair the injured blood vessel. What we don’t want is clots forming where they are unnecessary; or getting large enough to occlude major vessels; or breaking off into little blood-clot pieces (emboli) that swim to and then clog up small vessels supplying important structures (like the eye or the brain, causing an embolic stroke).
Too much bleeding and too much clotting are both problematic; we have to get the balance Goldilocks-level right, or suffer the consequences. You can see why this complex process is important enough to feature on every medical exam.
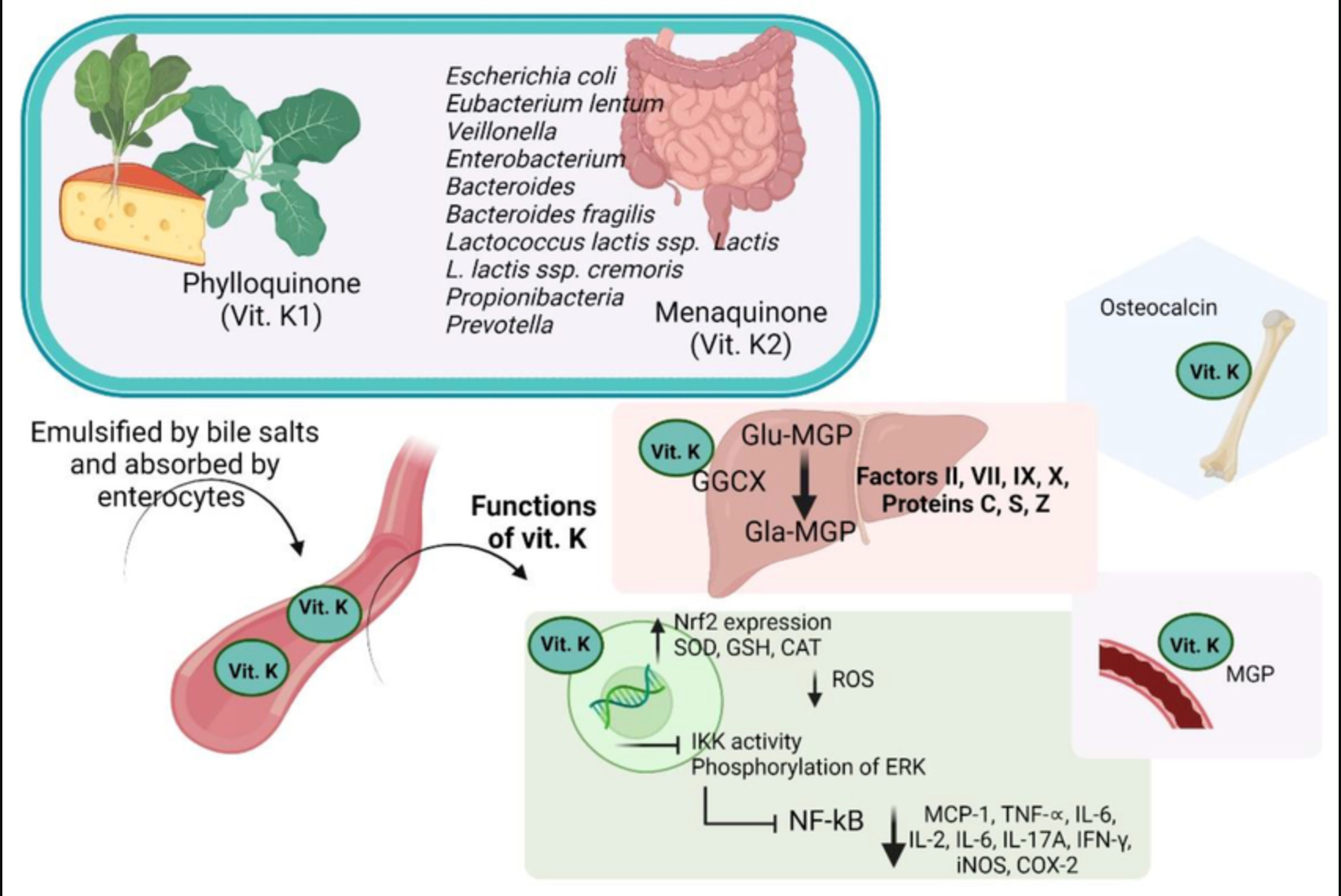
Several of these annoyingly named pro-coagulant and anti-coagulant factors can’t function without Vitamin K as a cofactor. These are: Factors 2, 7, 9 and 10, which are anticoagulant (help promote bleeding) and Proteins C and S, which are procoagulant (help promote clotting). Without Vitamin K, these factors are released into the bloodstream in an inactive form.
We first learned about Vitamin K when Henrik Dam, a biochemist from Copenhagen, postulated that a fat-soluble substance necessary for ‘koagulation,’ existed (which he thus named Vitamin K) by observing that chickens fed a fat-free diet developed spontaneous bleeding. In 1943, he won the Nobel Prize for his breakthrough, along with American biochemist Edward Doisy, who identified the chemical structure in 1939. Isn’t it great to support scientific discovery?

Vitamin K sources
There are several forms of Vitamin K. Phylloquinone, or Vitamin K1, is the most common source for humans, and the major dietary source. You can find it in delicious leafy green vegetables like Brussels sprouts, kale, and lettuce. Vitamin K2, or menaquinone, is found in some animal and fermented products, and is also made by intestinal bacteria.
Babies are not adults, though
Babies have low vitamin K levels for several reasons. There is not much passage of vitamin K through the placenta (so levels at birth are low) nor in breastmilk (so levels stay low, even in parents trying to increase their vitamin K). Obviously, they are not eating leafy greens at birth so vitamin K1 is limited to what they get from the placenta and through breastmilk.
They also lack the vitamin K2 that is synthesized by bacteria colonizing the gut. Babies don’t have that bacteria all settled in at birth; the neonatal microbiome takes time to fully establish and is affected by parental microbiome, mode of delivery, and other postnatal factors (such as use of antibiotics). So overall, babies are starting with low levels of Vitamin K.
Additionally, babies, and especially preterm babies, have very different levels of the coagulation (both pro- and anti-coagulant) factors in their blood. Coagulation factors can’t cross the placenta; the fetus starts making their own bleeding and clotting factors as early as 5 weeks and they are measurable by 20 weeks.
Still, babies are not adults. By the time of term birth, most coagulation factor levels in babies are much lower than adult levels, and only normalize by around 6 months of age. Some factor levels, however, are similar or even higher than in adults after birth! (This is why I love neonatology.) We use age-based reference ranges when evaluating coagulation parameters for infants; these are pretty suboptimally defined for extremely preterm infants (since most of them have some degree of clinical illness and thus hematologic derangement which affects our ability to establish ‘normal’ reference ranges).
Deficiency in vitamin K, an immature microbiome, poor transmission of vitamin K in breastmilk, and abnormal levels of clotting factors: this is a setup! There will be blood.
All of this is why, prior to universal vitamin K supplementation at birth, babies were afflicted by severe bleeding. Hemorrhagic disease of the newborn was recognized for ages but was first medically described in 1894 by a doctor who followed 50 babies with generalized bleeding in their first week of life; 60% of them died. These were regular infants who did not have traumatic deliveries or ongoing hematologic diseases (such as hemophilia). After the AAP recommended universal vitamin K supplementation, cases of hemorrhagic disease of the newborn or vitamin K deficiency bleeding became so rare that occurrences get published as case reports.
Hemorrhagic Disease of the Newborn aka VKDB (Vitamin K Deficiency Bleeding)
We know more about VKDB now than we did in 1894. Specifically, we know there are three types, all of which are also annoyingly named:
Early VKDB:
Timing: at birth-1 day
Presentation: rare, life threatening; ranges from bruising to intracranial and internal bleeding
Cause: maternal vitamin K deficiency; often due to medications interfering with vitamin K and inducing the CYP450 enzymes in the fetal liver (antibiotics, anticonvulsants, warfarin, anti-tuberculosis)
Prevention: unfortunately, supplementing vitamin K prenatally has shown higher umbilical cord vitamin K concentrations, but not a lower rate of Early VKDB
not enough evidence currently to recommend prenatal vitamin K supplementation to people taking these medications
though no clear data saying not to, so worth a try - talk to your doctor!
Classical VKDB:
Timing: first week of life
Presentation: GI bleeding, bleeding from umbilical stump, bleeding from circumcisions
some places will not let a baby get circumcised without having gotten a vitamin K shot
Cause: idiopathic (aka we don’t know the exact mechanism)
Prevention: Vitamin K shot; oral vitamin K may work
Late VKDB:
Timing: >8 days until 6 months (!) of life; peak 3-8 weeks
Presentation: variable but can be severe. Many with intracranial hemorrhage (some fatal), mucosal bleeding (bloody stool, urine, nose, gums, belly button); rare cases of bleeding in the eye (!!) or the thymus
outcomes range from no lasting effect to severe developmental delays to death
Cause: idiopathic in some cases; but can be associated with disease states with poor absorption (cystic fibrosis, short gut, liver disease, biliary atresia). These occur in children whose parents refused the vitamin K shot.
Prevention: Vitamin K shot; oral vitamin K does NOT WORK well enough

Treatment for VKDB
The best treatment is prevention. Your baby never has to get VKDB! You can worry about everything else in their life, except this, once they received the vitamin K shot.
Treatment is supportive. We give vitamin K to help the clotting factors that are there, transfuse blood products as needed, support circulation with medications that help support heart contractility and blood pressure, and treat any bleeds that are too big through neurosurgical procedures such as decompression and drain placement. And we hope it works. Not all damage is reversible, especially in cases of intracranial bleeds.
Recommended VKDB prevention
So let’s never do that. Let’s avoid VKDB by following the AAP recommendation, which is one shot, within 6 hours of birth, of 0.5 to 1.0 mg vitamin K. This single injection in the thigh provides a sustained release of vitamin K until the infant’s coagulation factor levels normalize, gut bacteria starts synthesizing Vitamin K2, and their diet expands to include dietary sources of Vitamin K1. Doses are slightly different in preterm infants but they also get a shot shortly after delivery (especially critical in preterm infants under 32 weeks who are at higher risk of intracranial bleeds at baseline - a topic for another issue of Babies, Explained, if you are interested - let me know!).
If only it were that simple. And it can be - wham, bam, thank you ma’am, for 6 months of protection against some pretty dire consequences. But studies show Vitamin K refusal continues to grow, spurred on by misinformed influencers (who probably have never cared for a baby with a catastrophic head bleed), and running exactly along the demographic lines you’d expect (vaccine hesitant, engaged in the appeal-to-nature fallacy).
Refusal is growing, and estimates show there is variation by location of birth. In hospitals, refusal rates are estimated from 0.2%-3% of all births; at birthing centers, they are 35% and for home births, 14%.
Let’s do some math: There were 3,667,758 births in the US in 2022. If even 3% of parents refused vitamin K, that is 110,032 babies who are at risk of VKDB.
Without the vitamin K shot, there are 250-1700 cases of early VKDB per 100,000 births and 10-80 cases of late VKDB per 100,000 births.
So in our example, each year, let’s say 50 babies have large intracranial hemorrhages from late VKDB (that were completely preventable). 50 may not seem like a lot, but think of it this way: if a comet fell to earth and hit a nursery of 50 infants, or contaminated formula killed 50 babies every year, it would be all over the news.

What happens when parents refuse Vitamin K
Some states strongly recommend vitamin K; other states require it. ‘Requiring’ means there are refusals, but those refusals involve the parents signing paperwork stating they understand and accept responsibility for severe bleeding, including intracranial hemorrhage. ‘Requiring’ also means that physicians (or other hospital staff) may need to make a report to the state and to the Department of Children’s Services about this.
I appreciate making this critical recommendation opt-out, and trying to maximize the number of people getting the shot. But there are costs too. In most hospitals I’ve worked at, a doctor is called after a family refuses vitamin K to go convince them.
I think I’m a reasonable person. I truly believe these families, despite the research (or influencer baloney) that has convinced them, are completely aligned with me in wanting the best for their child. But I also know that trying to bang someone over the head with evidence, especially on such a precious day, and also accusing them of basically being ignorant jerks, does not restore faith in the medical establishment. Nor does it a therapeutic doctor-patient relationship make.
If all medical decisions came down to quality of data alone, if we were purely rational beings, no one would ever smoke, people would wear helmets for every activity besides sleeping, we would all use shower chairs, and I would not have a crippling addiction to Cheezits. So I find these conversations a corrosive waste of everyone’s time (with extremely rare exceptions when people want to change their minds - key word - want. It is not my golden words that prompt this).
Reporting them to the Department of Children’s Services is a further waste of scarce resources, and a scare tactic that further entrenches people’s mistrust in the medical system. I keep my mandated conversations brief; I am always ready to answer questions in good faith, based on my knowledge of the evidence and years of experience. But I can only convince the convince-able.
Parent FAQ:
I hope I've convinced you that Vitamin K Deficiency Bleeding is both terrifying and preventable. While there are many aspects of parenting that involve difficult decisions and trade-offs, this shouldn't be one of them. The vitamin K shot represents one of modern medicine's best success stories: a single intervention that prevents devastating outcomes with minimal risk.
Below are common questions I hear from parents. If you're expecting a baby or know someone who is, please share this information to help ensure more babies are protected.
Should I supplement Vitamin K while I am pregnant?
Eat a nutritious diet (as best you can), take prenatal vitamins (hopefully begun long before you are trying to conceive), and talk to your doctor.
There is insufficient data to recommend supplementing Vitamin K prenatally, even for those taking medications like anticonvulsants, but your OB will be able to help you manage other nutrients you may need to supplement (e.g. folate).

Are there any risks of the Vitamin K shot?
Very few! As with any shot there is some risk of pain, but honestly most babies move on within seconds, and appear just as bothered by other annoyances like changing their diaper.
What can we do to minimize pain?
You can hold your baby, let them suckle, talk or sing to them while they get this shot (and any other shot moving forward) - all of these are evidence-based methods to reduce pain without medications.
What about oral vitamin K? I hear it’s used in Europe!
Oral vitamin K is used in many European countries. Three points you need to know about that:
Regimens, like health systems, vary by country. Most of these regimens require multiple doses, ranging from 3 dose regimens in several European countries to a new 13 dose regimen found to be superior to them in a recent paper in Japan.
These countries have the capacity for better follow-up, including home visits from nurses, more frequent pediatrician visits (and hoo boy, far better parental leave policies) than we do in the US.
Unfortunately, none of these regimens are superior to the one-time shot! They just aren’t. They reduce but do not eliminate the risk of late VKDB.
Even if you insisted, there is no FDA-approved oral version of vitamin K in the US. It would be made from crushed pills by a compounded pharmacy or just the IV version but by mouth. I do not recommend and would not prescribe that.
Is there a risk of cancer?
There is not, as far as the data shows. One study in 1990 found an association (not a causation!) with leukemia; extensive later studies refuted that and failed to demonstrate this association. But you didn’t need me to tell you that - if 3.66M babies each year were being exposed to something carcinogenic, it would be impossible to hide.
What about the preservative?
There are tiny amounts of benzyl alcohol and aluminum and other preservatives in some vitamin K shots; all are at doses that are below the levels for toxicity.
What would I do if it was my child?
Worry about so many other hideous things happening right now. The erosion of environmental, food safety, and medical protections are a real concern, as is the loss of reproductive freedom. There are so many other things to panic about! But Vitamin K has an excellent track record at being safe and saving lives. I would give my baby the injection and not waste a single moment worrying about this when there’s such a better menu to choose from.
Where can I learn more about vitamin K?

Thanks for being here, my friends! I am so grateful you are here. If you found this helpful, please click the ❤️ button - it would make me feel like I am not shouting into the void. ☕If you’d like to help me, you can buy me a coffee, or re-stack this post so others can learn too.
This week’s highlights:
Reading: Fourth Wing. (Loving it so far, but everyone says it keeps getting worse as the series goes on, so uh-oh). Just finished the Cher memoir, which both had plenty of tea and was inadequately introspective.
Watching: Finished Season 2 of Traitors. Allan Cumming’s wardrobe is everything. So is his dog. (His memoir was excellent, btw!).
Substacks I’m still thinking about: this piece by
about what happens when your daughter is treated like trash, by boys; this piece by which I think contains the answer to Ryan’s question (also read this piece to become indomitable); writing about the Overton Window, which is how we end up with all this anti-vax baloney and people feeling ok saying terrible things to women.Animal of the week: This porcupine climbing to get a sweet potato!

REFERENCES
Gianna M. Guzzardo, Katherine Regling; Developmental Hemostasis: The Evolution of our Coagulation System. Neoreviews February 2022; 23 (2): e82–e95. https://doi.org/10.1542/neo.23-2-e82
Rogers TP, Fathi O, Sánchez PJ. Neonatologists and vitamin K hesitancy. J Perinatol. 2023 Aug;43(8):1067-1071. doi: 10.1038/s41372-023-01611-w. Epub 2023 Jan 27. PMID: 36707666.
Stachowiak A, Furman L. Vitamin K Is Necessary for Newborns. Pediatr Rev. 2020 Jun;41(6):305-306. doi: 10.1542/pir.2019-0146. PMID: 32482696.
Hand I, Noble L, Abrams SA; AAP Committee on Fetus and Newborn, Section on Breastfeeding, Committee on Nutrition. Vitamin K and the Newborn Infant. Pediatrics. 2022;149(3):e2021056036
Loyal J, Taylor JA, Phillipi CA, Goyal NK, Wood KE, Seashore C, King B, Colson E, Shabanova V, Shapiro ED; BORN investigators. Factors Associated With Refusal of Intramuscular Vitamin K in Normal Newborns. Pediatrics. 2018 Aug;142(2):e20173743. doi: 10.1542/peds.2017-3743. PMID: 30030367; PMCID: PMC6317553.
Takahashi D, Egami N, Ochiai M, Hotta T, Suga S, Ishimura M, Kawaguchi C, Uchiumi T, Nishikubo T, Nogami K, Goto K, Ohga S. Vitamin K prophylaxis in neonates: comparing two different oral regimens. J Perinatol. 2024 Oct;44(10):1491-1495. doi: 10.1038/s41372-024-01981-9. Epub 2024 Apr 27. PMID: 38678081.
Osterman MJK, Hamilton BE, Martin JA, Driscoll AK, Valenzuela CP. Births: Final data for 2022. National Vital Statistics Reports; vol 73, no 2. Hyattsville, MD: National Center for Health Statistics. 2024. DOI: https://dx.doi.org/10.15620/cdc:145588
*
Disclaimer: The content provided in Babies, Explained is for educational and entertainment purposes only. It is not intended as medical advice, diagnosis, or treatment. It does not establish a doctor-patient relationship. Always consult with your healthcare professional regarding any medical concerns or decisions. The views and opinions expressed here are my own and do not represent the positions, policies, or opinions of my employers or any affiliated organizations. While I strive for accuracy, the information presented here may not apply to your unique situation.